Ct Scan Orbital Floor Mesh

Reconstruction Of Orbital Floor For Treatment Of A Pure Blowout Fracture Sciencedirect

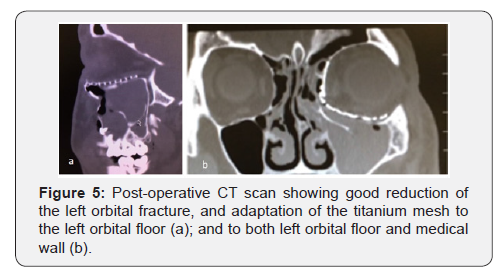
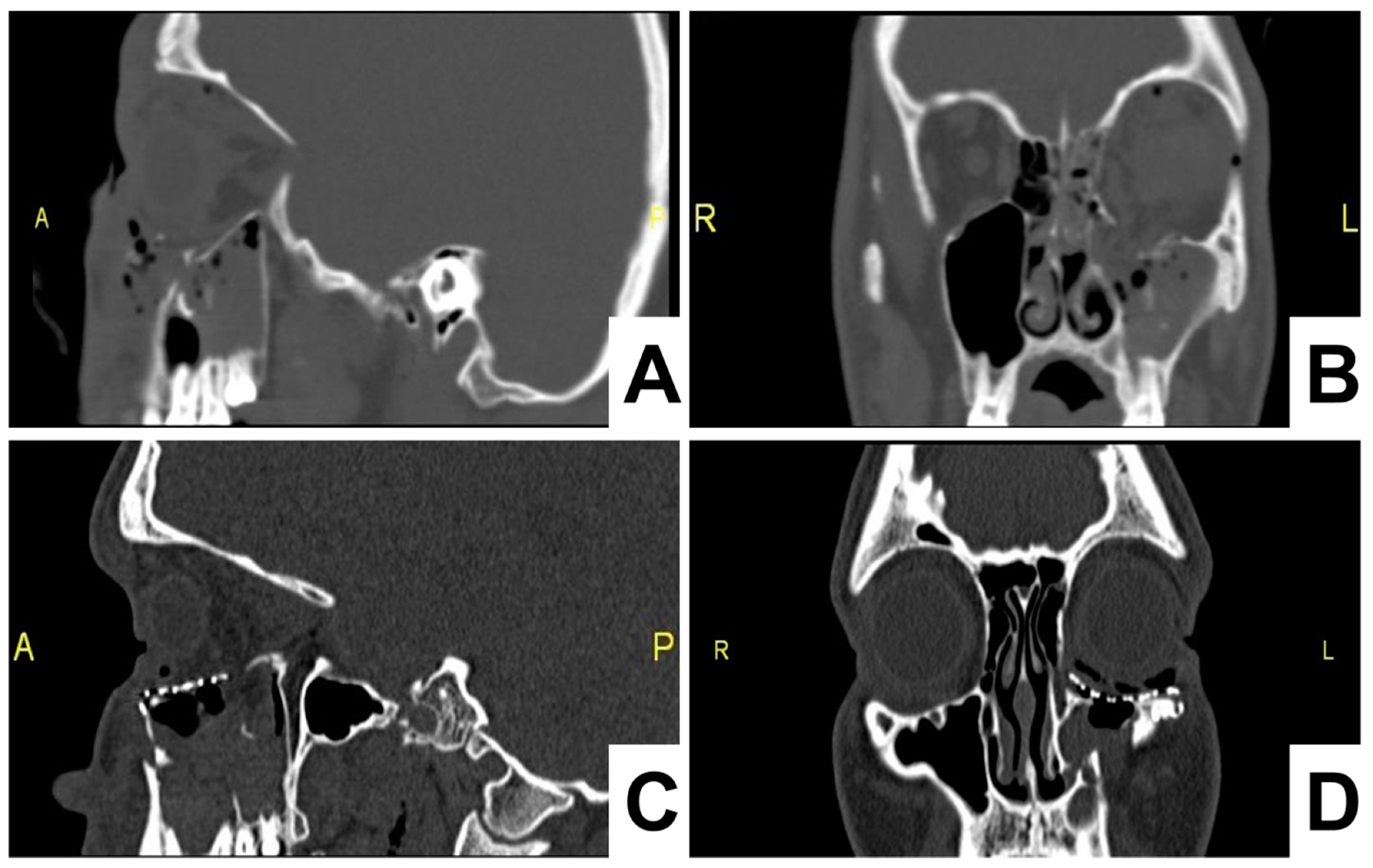
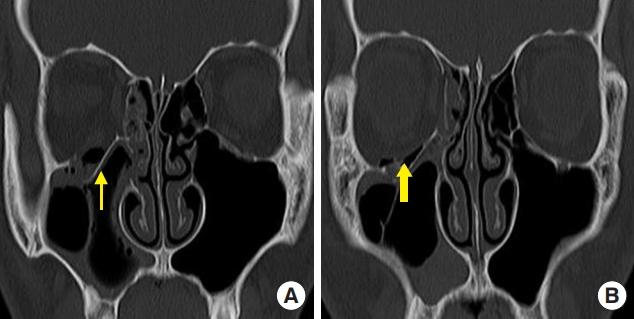
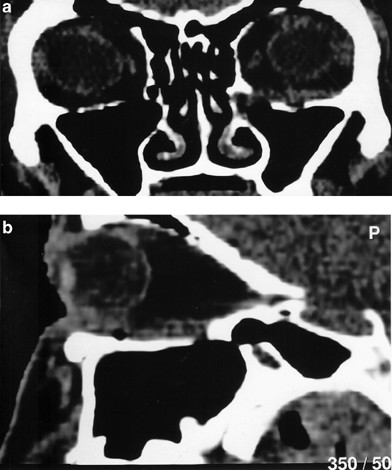
The Preoperative A And Postoperative B Ct Of The Left Orbital Floor Download Scientific Diagram

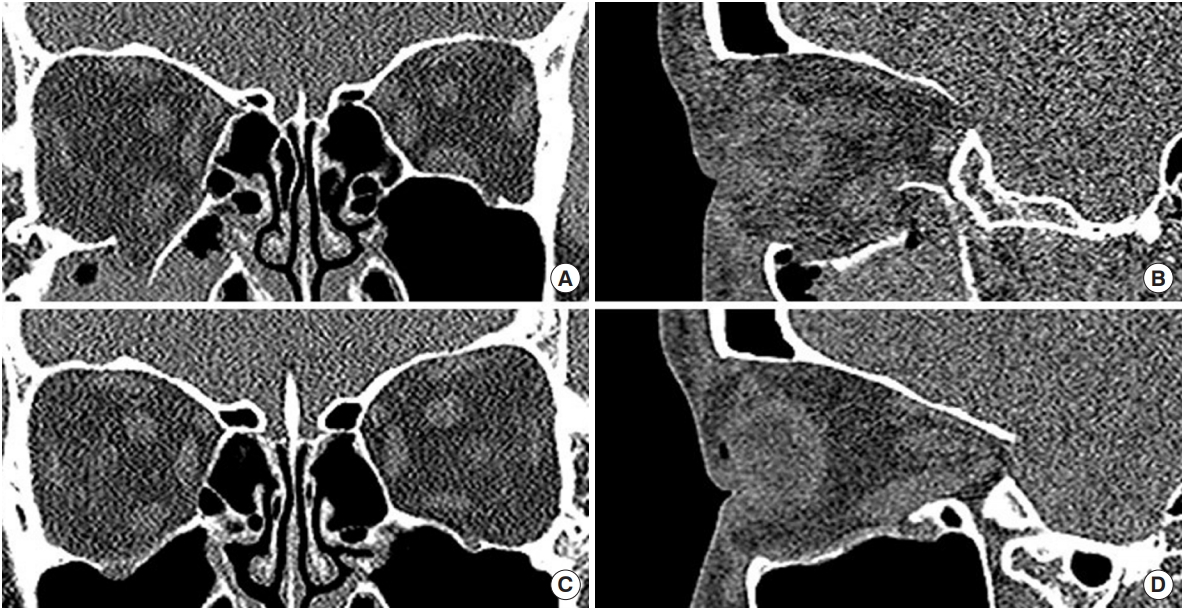
Group 1 Conv Ct Scan Images Of Patients With Unsatisfactory Orbital Download Scientific Diagram
Orbital Fractures

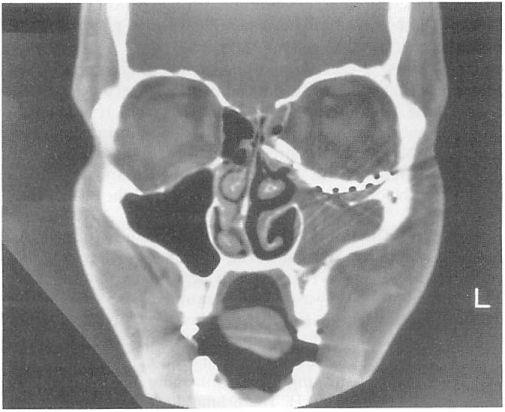
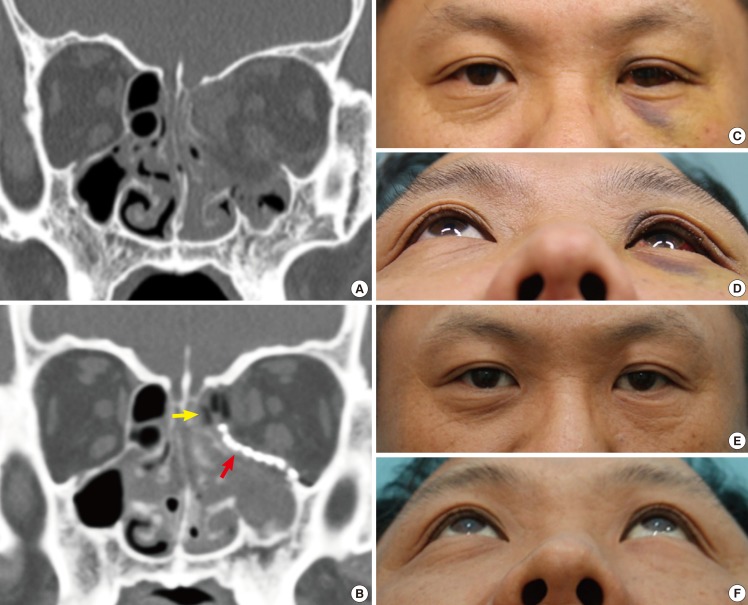
A Coronal Ct Scan Of The Patient Showing The Left Orbital Floor Download Scientific Diagram
Complex Orbital Fracture Repair Using Rigid Fixation Of The Internal Orbital Skeleton World Renowned Bespoke Cosmetic Plastic Surgeon Boston Dr Michael Yaremchuk
For most orbital fractures the imaging study of choice is ct scan.
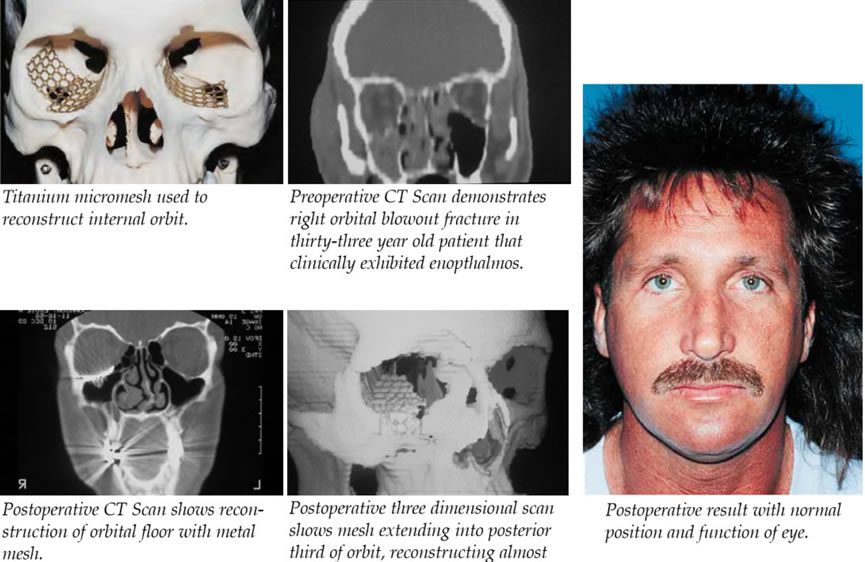
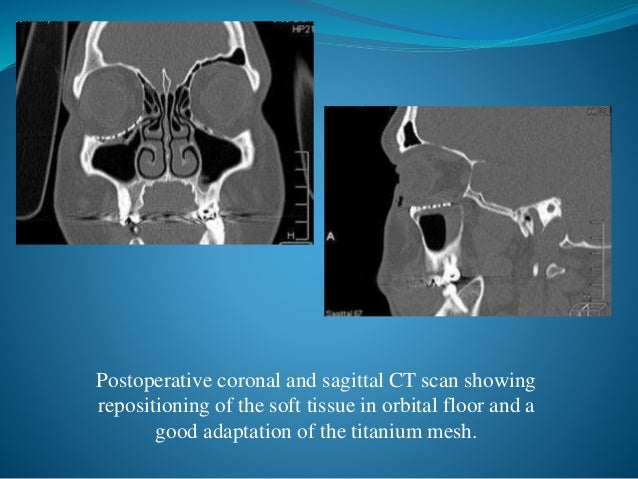
Ct scan orbital floor mesh. For minimal bending and cutting which reduces the amount of time. Orbital fractures pose specific challenge in its surgical management. Surgical treatment was performed using subciliary inferior palpebral approach to explore the orbital floor and placement of the titanium mesh and an intraoral antrostomy for endoscopy to magnification of the surgical field and adaptation of the mesh. Postoperative ct scan analysis shows that all treatments restored orbital volume and.
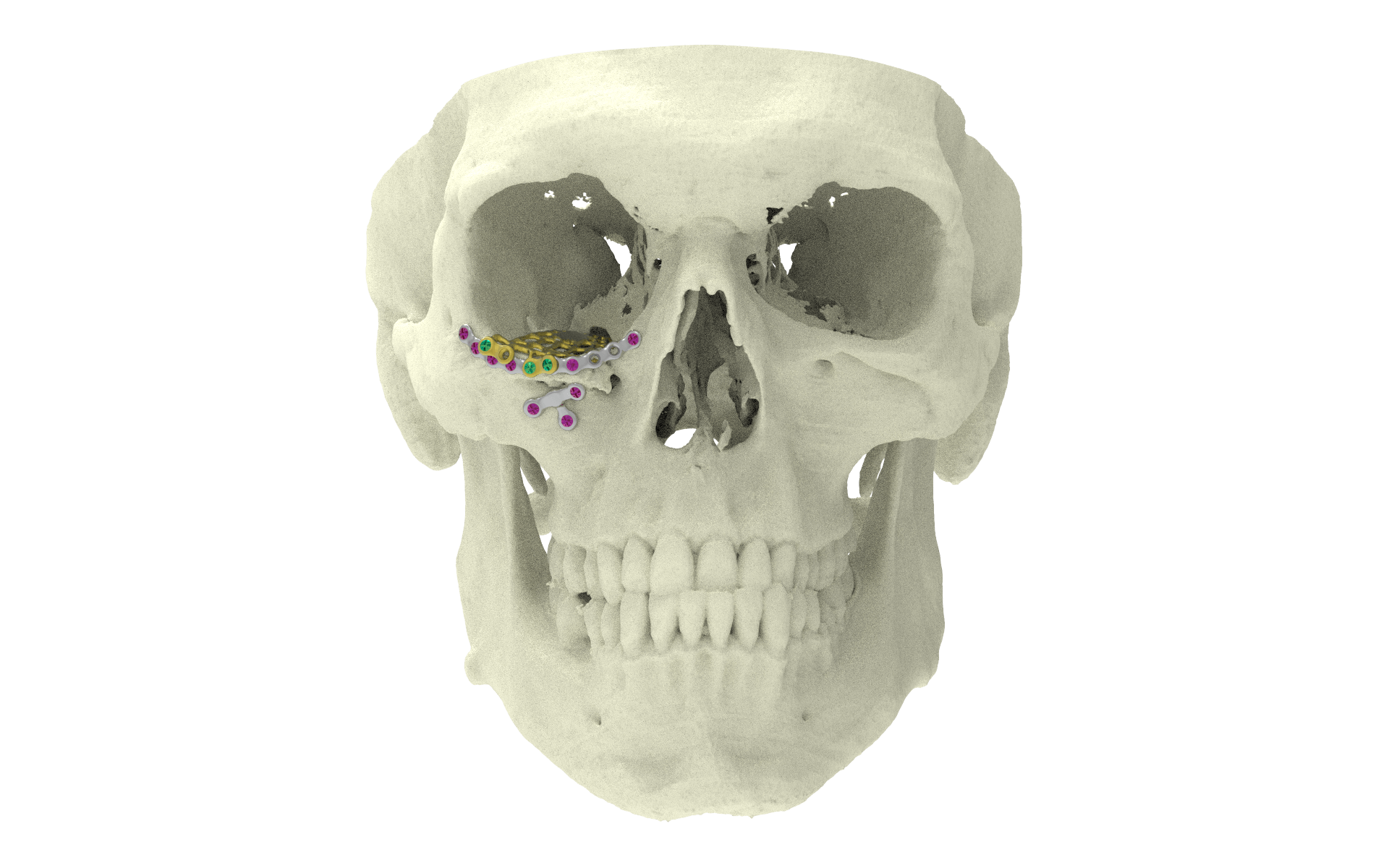
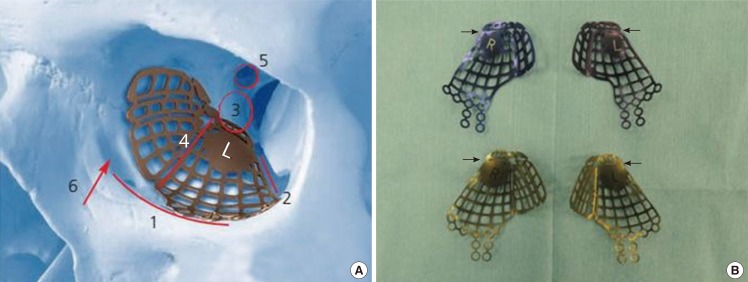
The overlying colored line in the medial wall and orbital floor area indicate the preoperative virtual planning that is superimposed on the mesh reconstructed area. In intervention group n 5 the ct scan slices were used for generating 3d reconstruction of both affected and unaffected orbits. 6 7 see the image below. The sagittal plane computed tomographic ct scan has been proposed as the most important radiologic view in the diagnosis of orbital floor fractures.
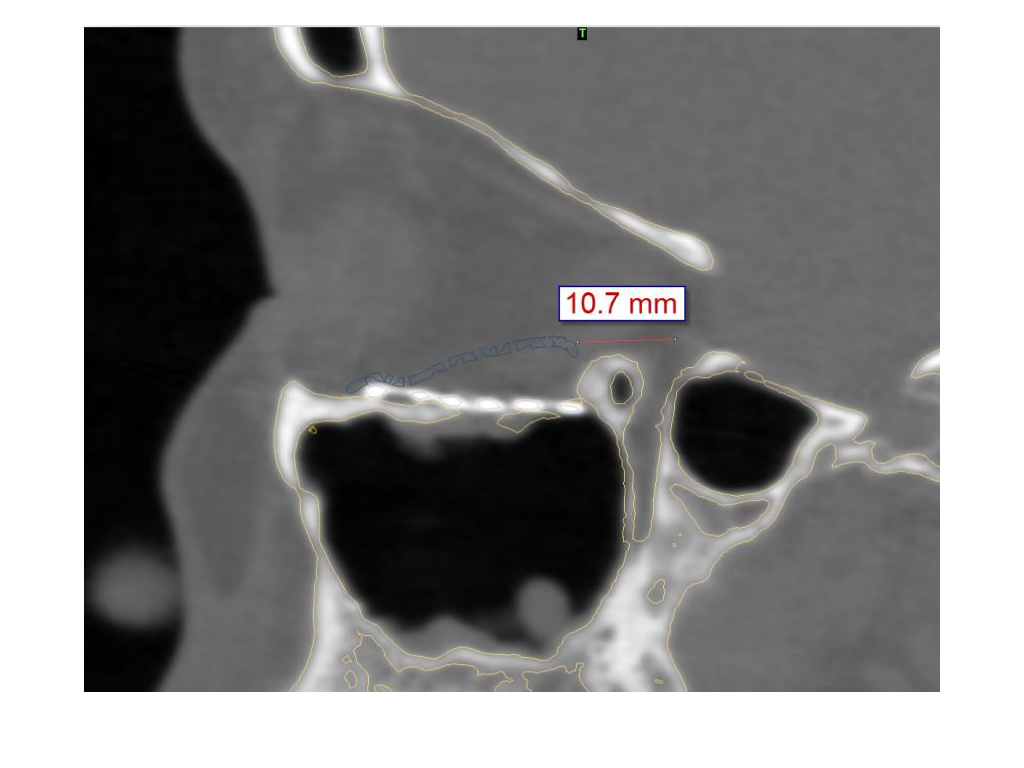
Psi placement over failed pre bend mesh. Coronal slice of a postoperative ct scan taken after transconjunctival repair of the complete left medial orbital wall and orbital floor. To design implants for orbital reconstruction rapid prototype models can be derived from digital imaging and communications in medicine dicom data obtained from the patient s computed tomography ct scan. In case the orbital floor is not properly reconstructed correction of shape and position of the implant is recommended followed by a.
The aim of this study was to describe t. This study was prospectively conducted on 10 patients with unilateral orbital floor fractures caused by accident or falls. Orbital floor designed from ct scan data the three dimensional implants closely approximate the topographical anatomy of the hu man orbital floor and medial wall to provide accurate recon struction even after significant two wall fractures 5 6 preformed three dimensional shape. This x ray shows the classic transition zone.
A ct scan with axial and coronal views is optimal. Before the advent of high resolution ct several articles were published in the radiology literature debating the need for direct sagittal views which required cumbersome patient positioning. One of the greatest challenges is to obtain satisfactory reconstruction by correct positioning of orbital implant. The matrixmidface preformed orbital plates are designed from ct scan data.
This confirms that there is no need for further corrections in this case. Ask for thin cuts 2 3 mm with specific attention to the orbital floor and optic canal.

Reconstruction Of Orbital Floor Using Titanium Mesh Download Scientific Diagram
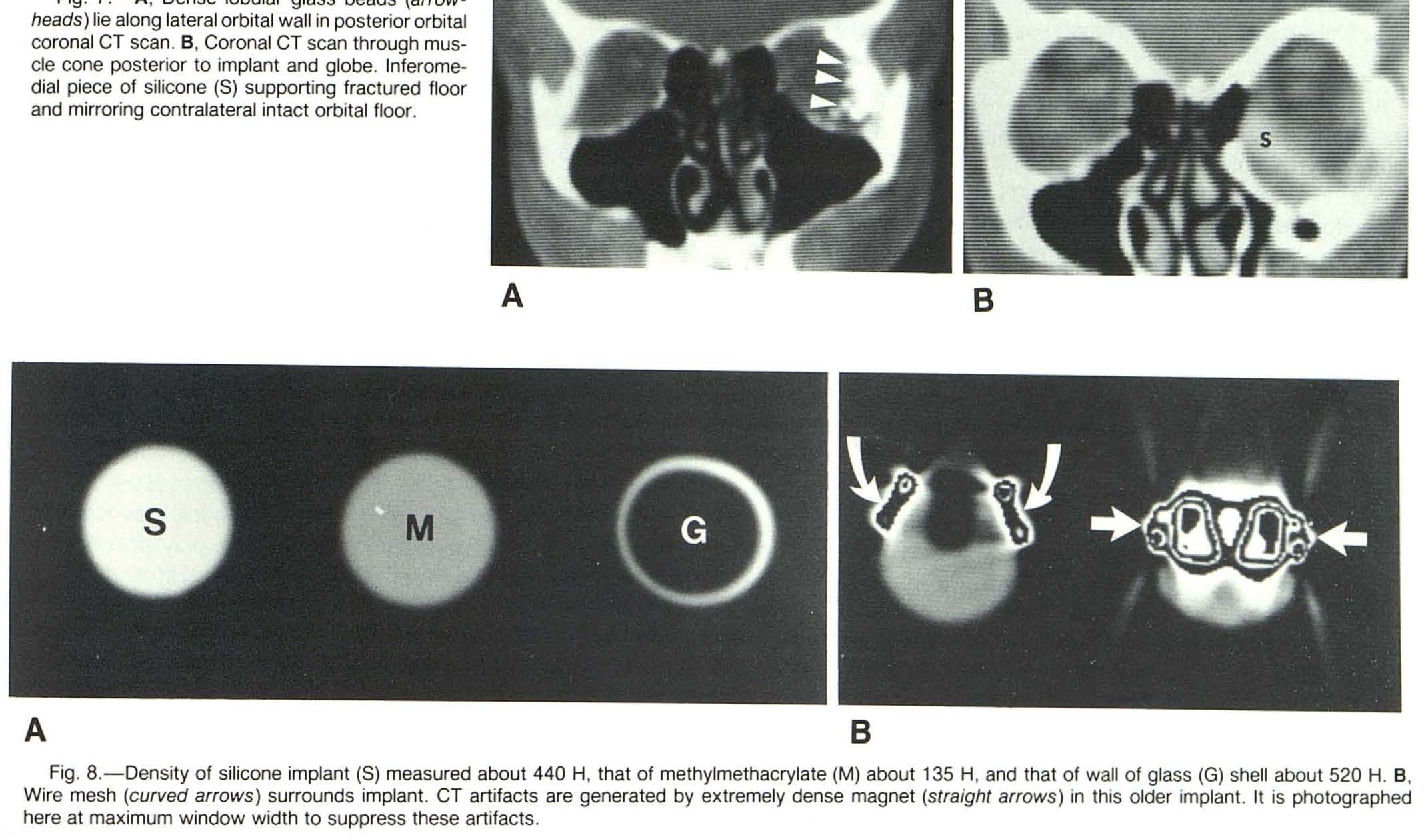
Pdf Orbital Implants And Prostheses Postoperative Computed Tomographic Appearance Semantic Scholar
Orbital Reconstruction Cas Virtual Planning And Intraoperative Navigation For Orbit Orbital Floor Fracture
Materials Free Full Text Periorbital Reconstruction By Periorbital Patch Technique Using A Pericardium Based Collagen Membrane And Titanium Mesh Html
Orbital Floor Xilloc
Orbital Reconstruction Cas Intraoperative Imaging For Orbit Orbital Floor Fracture
Combined Orbital Fractures Surgical Strategy Of Sequential Repair

13 Orbital Floor Fracture Plastic Surgery Key

Type Ii Fracture A Preoperative Ct Indicated Right Orbital Floor Download Scientific Diagram
Orbital Wall Restoring Surgery With Resorbable Mesh Plate
Orbital Floor Blow Out Fractures
Epos Trade
Journal Of Otolaryngology Open Access Journals

Application Of Three Dimensional Printing Technology In Orbital Floor Fracture Reconstruction Abstract Europe Pmc

The Role Of The Dentist In Recognizing Orbital And Ocular Trauma
Biodegradable Implants For Orbital Wall Fracture Reconstruction
Http Www Ajnr Org Content 6 3 403 Full Pdf
The Silent Sinus Syndrome A Collaborative Approach Between Rhinologists And Oculoplastics Case Report And Literature Review

Nhdogou2hzgx4m
Orbital Floor Fracture An Unusual Late Complication Eye
Three Dimensional Pre Bent Titanium Implant For Concomitant Orbital Floor And Medial Wall Fractures In An East Asian Population

Pdf Management Of Orbital Fractures Challenges And Solutions

Clinical And Epidemiological Characteristics Of Orbital Floor Fractures Rebuilt With Titanium Mesh

Pdf Orbital Floor Fracture Reconstruction Using Conchal Auricular Cartilage Graft
Pdf Update On Orbital Reconstruction
Endoscopic View Of The Orbital Floor From The Maxillary Sinus Notes A Download Scientific Diagram

Use Of Cad Based Pre Bent Implants Reduces Theatre Time In Orbital Floor Reconstruction Results Of A Prospective Study Sciencedirect

Customized Titanium Reconstruction Of Post Traumatic Orbital Wall Defects A Review Of 22 Cases Pocket Dentistry

Orbital Tumors Beverly Hills Los Angeles Eye Surgical Treatment

Pdf The Anatomage Table And The Placement Of Titanium Mesh For The Management Of Orbital Floor Fractures

Orbital Fracture Repair Abstract Europe Pmc
Epos
This Eye Does Not Look Right Ppt Video Online Download
The Curious Case Of The Hairstylist With Hyperglobus And Hypoesthesia American Academy Of Ophthalmology

Pdf A Novel Method Of Orbital Floor Reconstruction Using Virtual Planning 3d Printing And Autologous Bone
Reconstruction Of Orbital Floor Fractures With Titanium Micromesh Our Experience Springerlink

Orbital Adherence Syndrome Following The Use Of Titanium Precontoured Orbital Mesh For The Reconstruction Of Posttraumatic Orbital Floor Defects Abstract Europe Pmc
Pdf Late Complication Associated With The Treatment Of Orbital Floor Fracture With Titanium Mesh
Pdf Repair Of Orbital Floor Fractures Our Experience And New Technical Findings

Intraoperative Imaging O Arm In Secondary Surgical Correction Of Post Traumatic Orbital Fractures Sciencedirect

Ijmdcr
Orbital Reconstruction For Orbit Orbital Floor Fracture

